Feature Image Credit: piaxby.com
Please note this article was published on March 24 2020 16:30 GMT+9:30 (ADL, Australia) and some information may be out of date (such as infection numbers) or have progressed (our scientists work fast!). The sources are linked throughout including some helpful definitions.
So chances are by now you have already heard about COVID-19 or the novel Coronavirus that is sending cities and countries into lock down. COVID-19 was first detected on December 12, 2019 in Wuhan, China. Since then, the virus has spread to 189 countries, infected >334,900 people resulting in >14,600 deaths and mass inconveniences from cruise ship to country-wide quarantines.
There are so many different aspects to discuss – where did the COVID-19 come from, why is it spreading so fast, are our politicians doing enough, quickly enough, to stop the spread, should I be concerned? And there are loads of great and reliable resources around to help answer these questions (see your countries health organisation or the World Health Organisation’s website, links at bottom of article). What I want to focus on is the scientific community’s response to this pandemic.
For the most up to date information on the COVID-19 pandemic please visit the WHO dashboard
In recent times there has been a lot of discussion within and around scientific communities concerning accessibility and transparency of data. This includes the paywalls that restrict those outside large institutions from easily accessing journal publications, the availability of raw data from publications, and transparency (or lack thereof) in the peer-review process. What I have found amazing about the COVID-19 outbreak is not only the sheer amount of data that has been generated in such a short period, but the transparency and openness with which that data has been shared with both the scientific and general public. Many journals and news organisations have made all their publications relating to COVID-19 open-access to allow anyone easy access to the newest information. The turn-around times for review and publication of these papers range from days to weeks, rather than the months usually anticipated. Many publishers have now been so inundated with COVID-19 related articles that there are not enough peer reviewers available to review the articles.
Other researchers have chosen to circumvent the journal publication process altogether, forgoing the lustre of another paper to list on their next grant application and instead have opted for speed and ultimate transparency making available their raw data and results on independent websites.
Of course, this increase in speed may result in less robust publications, but across the board there is a general agreement that acting swiftly is more important than the usual slow march of scientific progress. This requires perhaps more caution in interpreting results, especially as a number of small sample size studies are published, however, these are all considerations that would always be taken into account by any diligent scientist.
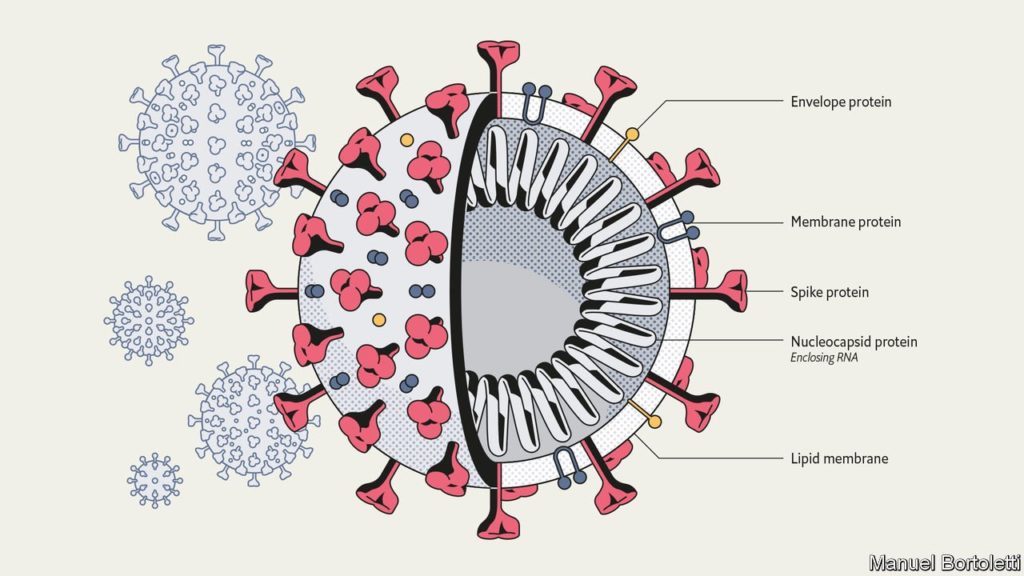
Briefly, what is SARS-CoV-2 (the virus) that causes COVID-19 (the disease)? SARS-CoV-2 is a virus formed of a lipid-bilayer with three key proteins embedded in the bilayer. One of these, the Spike protein recognises the ACE2 receptor (a protein highly expressed on our lung cells) facilitates entry of the virus into our cells. Encapsulated within the viral particle is an RNA transcript which codes for a number of proteins. Once the virus is in our cells, the RNA is translated by our cellular machinery, forming copies of these proteins which spontaneously assemble into more viral particles. The new viral particles are then able to spread and infect more people when expelled through respiratory droplets.
Although there is currently a lot going on, and it is reasonable to be concerned, let’s discuss some of the science. Here is a summary of some of the scientific advancements from the scientists working hard to combat COVID-19, a list which is by no means exhaustive.
Identification of COVID-19 & genome characterisation: The complete SARS-CoV-2 genome was published on January 10, under a month from the first case. This is a huge feat that would not have been possible only a few years ago when genome sequencing was still new. This information allows scientists to figure out where the virus came from, how different/similar it is to other viruses we know about, and express the virus proteins in the lab to discover effective drugs or develop vaccines.
The genome confirms the virus was definitely of natural origin, but we’re still not entirely sure which animal it first originated in or what facilitated the jump into humans.
Development & implementation of a test for diagnosis of COVID-19: The World Health Organisation (WHO) have developed and distributed the protocol for a real-time PCR test to allow diagnosis of COVID-19. This involves taking a swab of a potentially infected individual that is then screened for any evidence of the viral RNA, using our new knowledge of the Sar-CoV-2 genome. The US Centre for Disease Control (CDC) has also developed a similar test.
Within the last week, an antibody test has now been developed that can indicate if you ever had COVID-19, whereas the rt-PCR test only indicates an active infection with SAR-CoV-2, but is yet to be deployed.
Identification, expression, isolation & crystallisation of key proteins: Four main proteins of SARS-CoV-2 have been isolated and crystallised: Spike, Envelope, Membrane & Main Protease. Each of these structures is particularly important to aid in the development of drugs to inhibit the interactions these proteins are involved in, which will consequently inhibit the function of the virus. Understanding the 3D shape of proteins gives us a lot of information about how they function.
The proteins and virus as a whole has been visualised spectacularly by a number of researchers including Fusion Animation and Brady Johnston utilising some of the 29 SARS-CoV-2 protein structures already in the Crystal Data Bank.
The first of these structures was published by Rao and Yang from ShanghaiTech University – an amazingly high resolution crystal structure (6LU7) of the ‘Main Protease’ complexed with a protease inhibitor N3.
A team from the University of Washington are using this structure in their gamified protein-drug design program Fold-it, where scientists and the public are encouraged to design new proteins to bind a target. The best candidates will be synthesised and experimentally validated.
Fragment-based drug screening: Many teams are screening ‘fragments’, very small molecules which can be pieced together to design a drug, both experimentally and computationally. The Walsh group in collaboration with the von Delft group from the UK have been targeting the SARS-CoV-2 main protease. They have made over 1500 crystals of the protease which have then been soaked with a drug fragment. If the fragments bind to the protein a co-crystal structure can be obtained. This has yielded over 58 hits which is a great step forward in finding a viable drug.
Other teams at the Weizmann Institute in Israel have used mass spectrometry to find molecule fragments or specific electrophiles that interact with the protease before submitting their hits to crystallographic analysis. This highlighted chloroacetamides as a promising lead for drug discovery, which may confer selectivity for this virus as they have not commonly been employed elsewhere.
PostEra are now crowd sourcing molecular design of potential drug candidates against COVID-19, you can go online and design a molecule using their fragments, giving reasoning for why you think it might be effective, and then it will be synthesised and tested.
Screening of existing FDA approved drugs: Repurposing of existing drugs, which have been shown to be safe to the human population, is a way to fast-track treatment of COVID-19. Several anti-virals and protease inhibitors that are used to treat malaria, flu or HIV, are being assessed.
Chloroquine (used to treat malaria & rheumatism) has been highlighted by in the media and is gaining some traction in the medical community. Chloroquine was trialled in France and appeared to be effective against COVID-19 infections among a small sample size. There are larger (though still small) clinical trials underway in Minnesota, as well as other locations.
A large collaboration (with a large San Franciso representation) have screened the interactome of SARS-CoV-2 to identify targets that could be drugged with exisiting compounds. The Scripps Research Institute is also screening existing drugs to combat COVID-19.
Modelling of COVID-19 spread: A large number of groups from the University of Adelaide, (Australia) to the Imperial College of London (England) are modelling the spread of COVID-19 to understand what we need to do to be able to contain the virus and what to expect next. This is no small feat with a huge number of variables to be considered and a constantly changing environment as new guidelines and regulations are put in place to stem the spread. These factors include travel patterns (locally & globally), population densities, the disease pathology such as when symptoms arrive, the infection and death rates, hygiene practices, natural immunity and ability of the healthcare system to cope with increasing numbers of patients. Here’s a simple diagram to describe how you staying in can help slow the spread of the virus:
Vaccine development: A number of groups have started the development of vaccines for COVID-19. A vaccine is the most effective way to deal with COVID-19 however this is many months away from wide-spread deployment. The Coalition for Epidemic Preparedness Innovations (CEPI) is at the forefront of the vaccine development and encompasses teams from the Universities of Queensland (Australia), Hong Kong (Hong Kong), and Oxford (England) and companies Pfizer and BioNTech. This vaccine does not contain any virus, but instead – an RNA transcript. The human cells will then transcribe the RNA and produce the viral protein encoded. This protein should be recognised by the immune system, thereby training it to recognise this small piece of SARS-CoV-2 and readying it for a potential future infection. The first phase 1 clinical trial began last week in Seattle. Phase 1 clinical trials are purely to test the safety of the vaccine in a healthy population, and not yet to assess the effectiveness of the drug. The ultimate goal would be to design a vaccine that protects against the corona-virus family as a whole to combat future outbreaks, and not just SAR-CoV-2. However, this is easier said than done, especially as these viruses are prone to mutations.
This is a brief overview of some of the key research being done concerning the COVID-19 outbreak. The sheer number of different universities from all over the world mentioned above demonstrates the global cooperation occurring to best COVID-19. In conjunction with this has been a huge push particularly on social media to engage and inform the general public and stem the spread of information around the virus. Hopefully, this impact will not be short-lived and will increase the scientific literacy of our population as a whole, and demonstrate that transparency and collaboration are effective and important for scientific advancement and implementation.
With that said – wash your hands, and if you don’t need to go out, don’t. Check your sources are reliable before sharing, call your family and friends and importantly, be kind to one another.

Sources are hyper-linked within the respective discussion. Some general resources are linked below:
Health
World Health Organisation COVID-19 Dashboard
European Centre for Disease Prevention and Control
National Institute of Health (USA) – Coronavirus
Australian Government Department of Health- COVID-19
Why self-isolation is important (UK gov)
Flattening the curve – Three phases of COVID-19
Science
Nature
Elsevier
Royal Society of Chemistry
Research Collaboratory for Structural Bioinformatics Protein Data Bank (RCSB PDB)